
Tumor Classification & Cancer Identification
Understanding tumor classification and cancer types is essential for effective cancer identification and treatment. Different cancers have distinct causes, progression rates, and responses to therapy, making proper classification vital for optimal care.
BLOGS-RATHBIOTACLANSTUDY ZONE
Tumor Classification and Nomenclature
Cancer Identification
Proper identification of a cancer is necessary for many reasons. Cancers vary by cause, rate of progression, pattern, and response to therapy.
Different cancers will have different causes, different rates and patterns of progression, and different responses to treatment. The classification starts with knowing the tissue and organ of origin, the extent of distribution to other sites, and the microscopic appearance of the lesion. Increasingly, it also includes a detailed description of the critical genetic changes in the cancer.
Characteristics of Benign Tumors
Benign tumors, which are not referred to as cancers, are usually encapsulated with connective tissue and contain fairly well-differentiated cells and well-organized stroma.
The retain recognizable normal tissue structure and do not invade beyond their capsule, nor do they spread to regional lymph nodes or distant locations. Mitotic cells are very rarely present during microscopic analysis.
Benign tumors are generally named according to the tissues from which they arise with the suffix “-oma,” which indicates a tumor or mass. For example, a benign tumor of the smooth muscle of the uterus is a leiomyoma, and a benign tumor of fat cells is a lipoma. Benign tumors of the colon or stomach usually present as colonic or gastric polyps, and those of melanocytes present as dark-colored nevi (e.g., birthmark, mole).
It is important to understand that benign tumors can become extremely large and, depending on their location in the body, can cause morbidity or be life-threatening by compressing normal tissue, preventing blood flow to the region (ischemia), or causing necrotic death of normal tissue. For example, a benign meningioma at the base of the skull may cause symptoms by compressing adjacent normal brain tissue.
Benign tumors of endocrine organs may lead to overproduction of hormones. Some tumors initially described as benign can progress to cancer and then are referred to as malignant tumors, which are distinguished from benign tumors by more rapid growth rates and specific microscopic alterations, including loss of differentiation and absence of normal tissue organization.
Characteristics of Malignant Tumors
One of the microscopic hallmarks of cancer cells is anaplasia, the loss of cellular differentiation. Malignant cells are also pleomorphic, with marked variability of size and shape.
They often have large darkly stained nuclei, and mitotic cells are common. Malignant tumors may have a substantial amount of stroma, but it is disorganized, with loss of normal tissue structure. Malignant tumors lack a capsule and grow to invade nearby blood vessels, lymphatics, and surrounding structures.
The most important and deadliest characteristic of malignant tumors is their ability to spread far beyond the tissue of origin, a process known as metastasis.
Naming Conventions for Tumors
Unlike benign tumors, which are named related to the tissue of origin, cancers are generally named according to the cell type from which they originate.
Epithelial Tissue Cancers: Cancers arising in epithelial tissue are called carcinomas. If they arise from or form ductal or glandular structures, they are named adenocarcinomas. For example, a malignant tumor arising from breast glandular tissue is a mammary adenocarcinoma, whereas an example of a benign breast tumor is a fibroadenoma.
Mesenchymal Tissue Cancers: Cancers arising from mesenchymal tissue (including connective tissue, muscle, and bone) usually have the suffix sarcoma. For example, malignant cancers of skeletal muscle are known as rhabdomyosarcomas.
Lymphatic and Blood-Forming Cancers: Cancers of lymphatic tissue are called lymphomas, whereas cancers of blood-forming cells are called leukemias.
However, many cancers, such as Hodgkin disease and Ewing sarcoma, are named for historical reasons that do not follow this nomenclature convention.
Carcinoma In Situ (CIS)
Carcinoma in situ (often abbreviated CIS) refers to preinvasive epithelial tumors of glandular or squamous cell origin.
Cancers develop incrementally, as they accumulate specific genetic mutations. Careful surveillance for cancer often detects abnormal growths in epithelial tissues that have atypical cells and an increased proliferation rate compared with normal surrounding tissues.
These early stage cancers are localized to the epithelium and have not penetrated the local basement membrane or invaded the surrounding stroma. Based on these characteristics, they are not malignant but are often called CIS.
Sites and Outcomes of CIS
CIS occurs in several sites, including:
Epithelial Tissues: Cervix, skin, oral cavity, esophagus, and bronchus.
Glandular Epithelium: Stomach, endometrium, breast, and large bowel.
In the breast, ductal carcinoma in situ (DCIS) fills the mammary ducts but has not progressed to local tissue invasion.
Fate of CIS Lesions
CIS lesions can have one of three fates:
Remain stable for a long time.
Progress to invasive and metastatic cancers.
Regress and disappear.
Challenges in Treating CIS
CIS can vary from low-grade to high-grade dysplasia, with the high-grade lesions having the highest likelihood of becoming invasive cancers. The time that such preinvasive lesions remain in situ before becoming invasive is unknown.
Some carcinomas of the cervix appear as preinvasive lesions in situ for several years before they progress to invasive carcinoma and metastatic tumors. Knowing how to best treat low-grade CIS lesions is challenging because the proportion that progress to cancer vs. the proportion that will never cause clinical problems is usually not known.
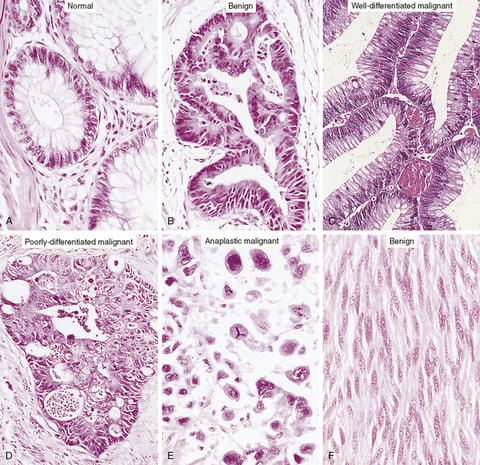
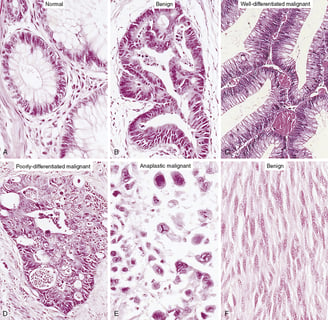
Loss of Cellular and Tissue Differentiation in Cancer Development
The benign neoplasm cells (B) resemble normal colonic epithelium (A) with an orderly arrangement, though mucin vacuolization is reduced. Well-differentiated malignant cells (C) form abnormal gland lumina with varied nuclear shapes. Poorly differentiated malignant cells (D) exhibit disordered arrangement and greater nuclear irregularities. Anaplastic malignant cells (E) lack resemblance to normal epithelium, with extreme size variation and hyperchromatic nuclei. Identifying the tumor origin microscopically becomes impossible. In contrast, well-differentiated tumors like the benign smooth muscle tumor (F) closely mimic their cells of origin.
credit :technology network
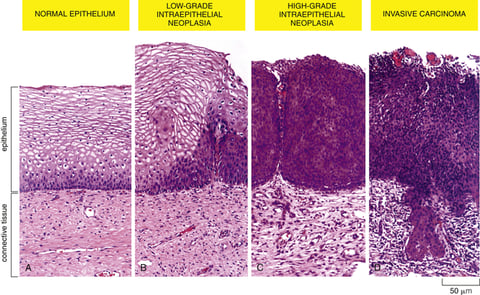
Progression from Normal to Neoplasm in the Uterine Cervix
Cervical cancer development follows a sequence of changes from low-grade to high-grade intraepithelial neoplasms (carcinoma in situ) and finally to invasive cancer. Early cervical neoplastic changes involve anaplastic cells and loss of normal tissue architecture, indicating cancer progression. Genetic abnormalities accumulate due to high cell division rates, local mutagens, and inflammatory mediators.
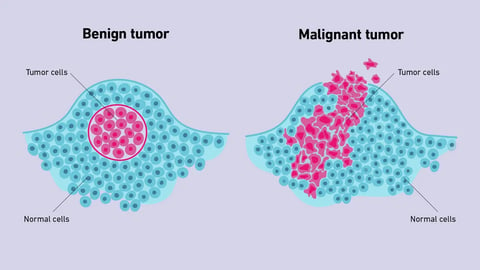
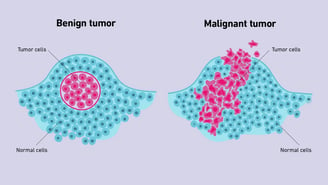
While benign tumors generally don’t invade and spread, malignant cells are more likely to metastasize, or travel to other areas of the body. They also grow faster.
ADVERTISEMENTS
ADVERTISEMENTS
ADVERTISEMENTS
ADVERTISEMENTS
ADVERTISEMENTS
ADVERTISEMENTS

Drop Us a Line
We’d Love to Hear from You