"CONNECTING RESEARCH TO REALITY"

Implantation Of Embryo In Humans
Implantation of embryo in humans is a complex process involving stages like migration, attachment, and invasion, crucial for establishing a successful pregnancy
STUDY ZONE
𝐒𝐇𝐈𝐁𝐀𝐒𝐈𝐒 𝐑𝐀𝐓𝐇
1/14/202512 min read
IMPLANTATION OF EMBRYO IN HUMAN
The term “implantation” is described as the process of attachment and invasion of the uterus endometrium by the blastocyst in placental animals.
It begins at the end of the first week and is completed by the end of the second week of gestation.
Implantation occurs in the endometrium of the uterus superior in the body region, slightly more often on the posterior.
It involves a receptive endometrium and hormonal factors such as estrogen, progesterone, prolactin as well as cell adhesion molecules, growth factors, and HOX (Hox genes are a group of genes that regulate the development of an animal's body plan, including the location of body parts) genes.
Further, the uterus is ready to accept the implanting embryo only during a limited period of time known as the ‘window of implantation’, outside of which the endometrium may be indifferent or even hostile to the embryo.
Site Of Implantation
The site of implantation is known as the particular position at which the blastocyst adhesions take place and subsequently implant inside the uterus. The uterus gives a favorable environment for embryonic development, and the site of implantation plays a vital role in the establishment of a successful pregnancy.
The blastocyst prefers the part of the uterus that is located at the fundus in most instances. The fundus is the top section of the uterus, meaning it is away from the cervical opening. The environment and conditions here are well endowed with blood supply and, thus, can support the implantation process on favorable grounds.
However, the implantation can be in other areas of the uterus. The other area where it can implant is the body of the uterus. This is the central part of the uterus that lies between the fundus and the cervix. The determination of where the blastocyst implants can vary with several factors, such as the characteristics of the embryo and the receptivity of the endometrium.
Some implant the blastocyst outside of the uterus while resulting in further complications and will, therefore, need a medical address. Ectopic pregnancies majorly occur along the fallopian tubes while can also appear on the ovarian end or sometimes inside the body's abdominal space.
The site of implantation is a result of the complex interaction between the blastocyst and the endometrium. The endometrium has cyclic changes in the menstrual cycle and becomes receptive for implantation at a particular phase called the receptive or "implantation window." The window of receptivity usually takes place between 6 to 10 days post-ovulation, which also coincides with the time the blastocyst reaches the uterus.
Understanding the site of implantation is of utmost importance in reproductive medicine and assisted reproductive technologies. In procedures such as in vitro fertilization, embryo transfer is done with utmost care to ensure implantation of the blastocyst at the best site within the uterus for implantation.
In conclusion, the site of implantation refers to the specific location within the uterus where the blastocyst becomes attached and implanted. The most common site for implantation is the fundus of the uterus, but the blastocyst can potentially implant in other areas of the uterus as well.
Implantation stages
Implantation is a complex process that involves a series of stages in the embryonic development of mammals. These stages are crucial for the successful attachment and invasion of the blastocyst into the uterine wall. The five recognized stages of implantation are migration and hatching, pre-contact, attachment, adhesion, and invasion. Let’s explore each of these stages:
Migration and Hatching: After reaching the uterus, the blastocyst undergoes migration within the uterine cavity. It moves and floats freely before hatching from the protective zona pellucida, a glycoprotein shell that surrounded the early embryo during its development in the fallopian tube.
Pre-Contact: During this stage, the blastocyst approaches the receptive endometrium, which is the lining of the uterus that has reached its optimal state for implantation. The blastocyst starts to make contact with the endometrial surface but does not yet attach.
Attachment: In this stage, the blastocyst firmly attaches to the endometrial lining. Specialized cells called trophoblasts, derived from the outer layer of the blastocyst, interact with the endometrium. These trophoblasts initiate the formation of the placenta, which will provide oxygen and nutrients to the developing embryo.
Adhesion: Once attached, the blastocyst further adheres to the endometrium, establishing a stronger connection. This adhesion is mediated by specific molecules and cell-to-cell interactions between the trophoblasts and the endometrial cells.
Invasion: The final stage of implantation involves the invasion of the trophoblasts into the endometrial tissue. This invasion allows the blastocyst to establish a close relationship with the maternal blood vessels and facilitate the exchange of nutrients and waste products. The depth and extent of trophoblast invasion vary among species, and it is a highly regulated process to ensure proper placental development.
It’s important to note that these stages occur within a limited timeframe known as the window of implantation. The uterus is only receptive to implantation during this specific period, which is influenced by hormonal changes and the cyclic nature of the endometrial lining.
Understanding the stages of implantation is vital for reproductive medicine and fertility treatments. Assisted reproductive technologies, such as in vitro fertilization (IVF), aim to optimize the timing of embryo transfer to align with the window of implantation, increasing the chances of successful implantation and pregnancy.
In summary, the process of implantation in mammals involves five recognized stages: migration and hatching, pre-contact, attachment, adhesion, and invasion. These stages are essential for the blastocyst to establish a secure connection with the endometrium and develop into a healthy pregnancy. The timing and success of implantation depend on various factors, including the receptivity of the uterus and the intricate interactions between the embryo and the maternal tissues.
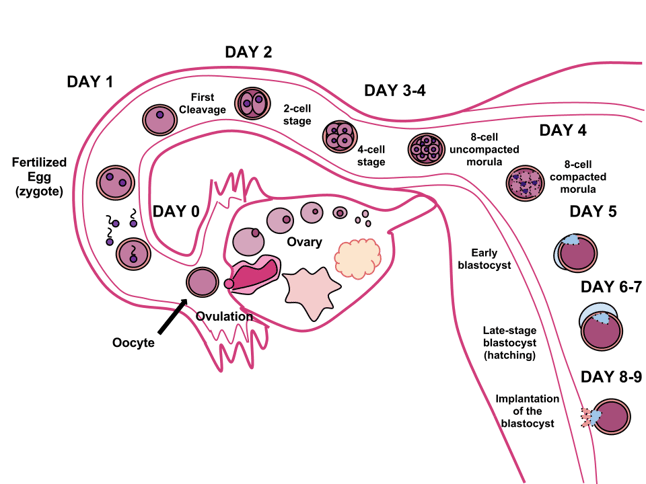
IMAGE CREDIT: WIKIPEDIA
ADVERTISEMENTS
ADVERTISEMENTS
Migration and hatching
Migration and hatching are the two important stages in the process of implantation during embryonic development.
Migration of the Zygote:
After fertilization occurs in the fallopian tube, the zygote undergoes migration towards the uterus.
Cilia lining the fallopian tube assist in the transport of the zygote.
In this migration, the zygote undergoes several cell divisions, and a compacted ball of cells called a morula is formed.
Migration of the Trophoblast:
As the morula enters the uterus, it undergoes further changes.
A cavity called the blastocoel forms within the morula, transforming it into a blastocyst.
The blastocyst consists of an inner cell mass that will develop into the embryo and an outer cell layer called the trophoblast, which will give rise to the extraembryonic membranes.
Zona Hatching:
The blastocyst is surrounded by a protective egg-coat called the zona pellucida. For implantation into the uterine wall, the blastocyst needs to break this coat. It is called zona hatching.
The lytic factors of the uterine cavity and the factors produced by the blastocyst itself break up the zona pellucida. Proteases stimulated by various growth factors are responsible for the dissolution of the zona pellucida.
Apposition:
Apposition is one of the crucial implantation stages. This stage is established after the blastocyst has hatched.
Apposition is defined as the primary loose contact or adhesion that the blastocyst makes with the endometrium of the uterus. This takes place at localized areas in the endometrium, usually at small crypts or invaginations. The degeneration of the zona pellucida enables the trophoblast layer of the blastocyst to contact the underlying endometrium directly.
During apposition, the inner cell mass referred to as the embryoblast orients itself nearest to the decidua which is the specialized uterine lining. The inner cell mass may freely rotate on the part of the trophoblast layer unless appropriately aligned with the decidua if it wasn't initially aligned.
Apposition is actually a weak association between the trophectoderm-the outer layer of cells of the blastocyst-and the uterine epithelium. It is an unstable interaction and vulnerable to shear stress. This interaction, being reversible, can move the blastocyst from one position within the uterus to another, as needed.
Apposition sets the stage for further stages of implantation, such as attachment, adhesion, and invasion, to take place. It serves as the initial point of contact between the developing embryo and the maternal tissues, paving the way for the establishment of a firm attachment and subsequent invasion into the endometrium.
Generally speaking, apposition represents the first loose contact between the blastocyst and the endometrium subsequent to zona hatching. It takes place in specific sites within the endometrium where direct contact between the trophoblast of the blastocyst and the underlying endometrium is achieved. Apposition represents a reversible and unstable relationship that provides the groundwork for future steps of implantation.
ADVERTISEMENTS
ADVERTISEMENTS
Adhesion
Adhesion is one of the important implantation stages, where the attachment between the trophoblast cells of the blastocyst and the endometrium becomes stronger.
During adhesion, the trophoblast cells penetrate the endometrium, making a more secure attachment than in the previous apposition stage. This penetration occurs through the extension of trophoblast cell protrusions into the endometrial tissue.
The surface of trophoblast cells is well endowed with numerous microvilli that play the key role during the adhesion process. Furthermore, binding fiber connections, laminin, type IV collagen, and integrins contribute to its adhesion into the endometrium.
The mucin-16 protein, also known as MUC-16, is expressed on the apical surface of the uterine epithelia. It acts as a barrier preventing the blastocyst from implanting in undesired locations on the epithelium. The removal of MUC-16 during the formation of pinopodes has been shown to promote trophoblast invasion in vitro.
The molecules that mediate the initial interaction between the trophoblast and the endometrial epithelia have not been identified. However, MUC1, a glycosylated protein belonging to the mucin family, has been suggested to be involved. MUC1 is expressed on the apical surface of endometrial epithelial cells during the window of implantation in humans. It has carbohydrate moieties that serve as ligands for L-selectin, a cell adhesion molecule that is expressed by trophoblast cells. There is evidence that L-selectin interacts with its ligands to mediate the apposition of the blastocyst to the uterine epithelium.
In summary, adhesion is more of an adherence between the trophoblast cells and the endometrium than apposition. This type of attachment results from the invasiveness of the trophoblast cells into the tissue of the endometrium, through which microvilli and other substances like MUC1 and L-selectin cause penetration. In this case, adhesion sets the stage for the following implantation stages such as invasion to take place.
Invasion
Invasive is the crucial implantation stage during which the blastocyst extends itself into the endometrium.
Invasion stage:
At this stage, the trophoblast cells, which had already attached themselves to the endometrium, start proliferating and further penetrate into the endometrial tissue. Penetration into the endometrial tissue is assisted by gelatinase A and B enzymes that break the extracellular matrix.
The main purpose of trophoblastic invasion is to gain access to maternal blood flow, thereby securing a vessel connection for fetal blood. When trophoblasts penetrate beyond some depth, they become terminally differentiated and will form a multinucleated tissue referred to as syncytiotrophoblast. The syncytiotrophoblast between the blastocyst and the endometrium and the cytotrophoblast around the inner cell mass.
It therefore dislodges the decidual cells when reaching the basal membrane beneath them in a continued invasion into uterine stroma.
These degradations are achieved in the cell adhesion molecules with their associated extracellular matrix to be dislodged. Through tumor necrosis factor-alpha, secretion is done from the syncytiotrophoblast into suppressing the expression of cell adhesion molecules and the beta-catenin. Further, the destruction of the matrix is done with various enzymes metalloproteinases and serine proteases.
As the syncytiotrophoblast invades the endometrium, it carries the embryo with it, eventually coming into contact with maternal blood vessels. This interaction leads to the formation of chorionic villi, marking the beginning of placentation.
After invasion, the breach created in the uterine epithelium by the blastocyst's entry is sealed by a fibrin plug, which consists of a coagulation of blood clot and cellular debris.
Extravillous trophoblasts invade the mother's uterine myometrium in addition to invading the endometrium. They remodel the spiral arteries to ensure better and more secured maternal blood flow to support the growing embryo. They can stabilize uterine veins to enable drainage of fetal blood and metabolic wastes.
During invasion, the blastocyst secretes numerous factors with different functions. Secretions include factors that stimulate autocrine effects for the stimulation of the blastocyst itself further to invade the endometrium, loosen decidual cells, and prevent rejection by the mother's immune system while triggering final decidualization as well as inhibiting menstruation.
The secretions by the blastocyst of immunosuppressive agents inhibit the immune system of the mother to reject the embryo. Such factors are platelet-activating factor, human chorionic gonadotropin, early pregnancy factor, prostaglandin E2, interleukin-1 alpha, interleukin-6, interferon-alpha, leukemia inhibitory factor, and colony-stimulating factor.
Human chorionic gonadotropin (hCG), one of the secreted factors, not only is an immunosuppressive agent but also signals to the mother's body that she is pregnant. This prevents luteolysis of the corpus luteum, sustaining its function and preventing menstruation.
Such factors also include histamine-releasing factor, tissue plasminogen activator, and its inhibitors, estradiol, β1-integrins, fibroblast growth factor, CYTL1, transforming growth factor alpha, inhibin, and preimplantation factor secreted by the invading blastocyst.
In summary, invasion is an important stage where trophoblast cells proliferate, penetrate the endometrium, and establish a deeper connection. This process involves the formation of syncytiotrophoblast, degradation of cell adhesion molecules and the extracellular matrix, and the eventual formation of chorionic villi. The invasion is accompanied by the secretion of various factors that support the implantation process, prevent rejection, and sustain the early pregnancy.
Process of Implantation of the Blastocyst in the Uterus
The process of implantation of the blastocyst in the uterus involves several stages that are essential for successful pregnancy. Let’s explore these stages based on the provided information:
Formation of the Morula: After fertilization occurs, the zygote undergoes rapid cell division, forming a solid ball of cells called the morula. This transformation takes place within the fallopian tube.
Transport to the Uterus: The morula takes approximately 3 to 5 days to travel through the fallopian tube and reach the uterine cavity. This transport is facilitated by a combination of fluid currents created by epithelial secretions and the beating motion of cilia lining the fallopian tube, which propel the morula toward the uterus. Weak contractions of the fallopian tube may also aid in this process.
Transformation into a Blastocyst: Within the uterus, the morula further develops into a blastocyst, which consists of approximately 100 cells. The blastocyst is a fluid-filled structure with an outer layer of cells called the trophoblast and an inner cell mass.
Implantation: The blastocyst spends 3 to 6 days freely floating in the uterine cavity before it becomes implanted in the uterine endometrium. During this time, the blastocyst relies on the nutritive secretions of the uterine endometrium, often referred to as “uterine milk.”
Trophoblast Action: Implantation occurs due to the activity of the trophoblast cells on the surface of the blastocyst. These trophoblast cells secrete proteolytic enzymes that digest and liquefy the adjacent cells of the uterine endometrium. This process allows the blastocyst to penetrate and anchor itself to the endometrium. Some of the fluid and nutrients released during this action are actively transported by the trophoblast cells into the blastocyst, providing additional nourishment for its growth.
Proliferation and Placenta Formation: Once implantation takes place, the trophoblast cells and adjacent cells from both the blastocyst and the uterine endometrium rapidly proliferate. This proliferation leads to the formation of the placenta and various membranes of pregnancy, which play crucial roles in supporting fetal development and maintaining pregnancy.
Receptivity of Uterus
The receptivity of the uterus also plays a pivotal role in this process of implantation. Such receptivity incorporates several changes into the endometrial cells and tissues that ensure the uterus to receive and subsequently support the conceptus.
This corresponds to the cellular changes of endometrial cells where receptivity presents with plasma membrane transformation. Formations such as formation of pinopodes, structures that resemble the mushroom protrudes from the cell membrane at uterine epithelial apices, represent ultrasrtructural and are formed around the window for implantation mostly between days 19 and 21 of GA.
Decidualization: The term decidualization describes the preparation of the endometrium for implantation. It involves thickening of the endometrium, vascularization, and growth of the glands. The endometrium also produces decidual cells, which form a new layer known as decidua, a layer that plays an important role in supporting and nourishing the developing embryo.
Window of Implantation: The window of implantation is a narrow window in time, when the endometrium is at its optimal receptivity to accept the implantation of the blastocyst. In human beings, it falls between the days 20 and 24 of the secretory phase of the menstrual cycle when luteinizing hormone is at peak levels. The window of implantation is only for 24 to 36 hours, which gives a sense of urgency to timing.
The receptor-ligand interactions during the window of implantation include important communication between the blastocyst and the endometrium. Receptor-ligand interactions, such as those of the integrin-matrix and proteoglycan receptors, contribute to this process. Proteoglycan receptors are on the surface of the decidua, and corresponding proteoglycans on the trophoblast cells of the blastocyst have these interactions contribute to adhesion and invasion into the endometrium.
Pinopodes: Pinopodes, which develop during the window of implantation, facilitate the receptivity of the uterus. They increase the absorption of uterine fluid, thereby decreasing the volume of the uterus and bringing the blastocyst closer to the endometrium. Pinopodes also facilitate direct contact and adherence between the blastocyst and the uterine epithelial cells, thus facilitating implantation.
Decidualization and Embryonic Influence: Decidualization is not only preparing the endometrium for implantation but also responding to signals from the developing embryo. Factors released by the blastocyst trigger the final formation of decidual cells and further changes in the endometrium. This interaction underlines the co-dependence between the viability of the embryo and the receptivity of the uterus.
Significance of Implantation
Implantation is one of the most critical steps in successful pregnancy, with several important considerations:
1. Failure of Implantation
Implantation failure is considered a primary reason behind unsuccessful pregnancies; it occurs in 85% of such failed cases. Such failures have resulted from one-third of inadequate uterine receptivity, whereas two-thirds relate to the issues concerning the embryos themselves. Failure also ranks topmost as one of the prime causes of in vitro fertilization setbacks.
2. Insufficient Uterine Receptivity
The ways by which uterine receptivity is impeded include abnormal cytokine and hormonal signaling as well as epigenetic alterations. The knowledge of these reasons can optimize endometrial receptivity with enhanced pregnancy success. Technologies including organ-on-a-chip systems, endometrial organoids, provide a greater insight into the understanding of endometrial function during implantation.
3. Improving Implantation Success
Implantation failure, which is recurrent, can be treated with low molecular weight heparin to improve live birth rates by 80% in assisted reproduction. Progesterone and hCG luteal phase support increases the chances of implantation as well.
4. Role of Zinc
Zinc is vital for pre-conception and successful pregnancy. Deficiency can impair blastocyst development and disrupt the zinc spark during fertilization, which is crucial for preventing polyspermy. Adequate zinc levels support healthy reproductive outcomes.
5. Implantation Bleeding
It occurs 7–14 days after fertilization, with light spotting, and it happens when the blastocyst embeds into the uterine lining, including symptoms like mild cramping, nausea, and breast tenderness. To differentiate it from menstrual bleeding, the flow characteristics of color, clotting, and duration should be assessed.
ADVERTISEMENTS
ADVERTISEMENTS

Drop Us a Line
We’d Love to Hear from You
RATHBIOTACLAN
Feel free to explore, engage, and embark on your own journey of discovery within RathBiotaClan. Together, let's make a difference in the world of Zoology_Bioscience !